VBCRM: Bridging Healthcare’s Greatest Divide

For a decade, healthcare has reached toward value while standing firmly on fee-for-service ground. The rhetoric has been aspirational; the reality is all about revenue.
While there’s widespread agreement and regulatory momentum to establish value-based care (VBC) as the future of healthcare, the fact is that 40.5% of payment today is pure fee-for-service (FFS), 19.5% is FFS with ties to quality and value, and 32.9% are APMs built on a FFS chassis. With only 7.5% of payment population-based, that means 92.5% remains tied to FFS.
This puts many health systems and physician groups in the complicated position of trying to succeed with two contradictory business models at once. For a small subset of their patients, the goal is to keep them healthy and out of the hospital while reducing overall costs through deft care management and coordination. But most of a health system’s book of business is based on attracting and treating people who are sick or injured and in need of the kind of costly acute care services and repeat business that generates revenue the old-fashioned way.
Not only are those business models in opposition, but so are the technology solutions many health systems deploy to support them. To manage the care of populations, health systems need data architectures that enable deep understanding of patient needs, predictive analytics, and seamless care coordination. In contrast, to attract patients for primary or acute care services, most health systems increasingly rely on standard enterprise customer relationship management (CRM) systems that have been modified for healthcare, often with little to no contextualized clinical data. While some legacy CRM vendors lightly fuel their CRM systems with microbial portions of clinical data, it's not readily usable or actionable. It’s just “there.”
Unfortunately, this platform schism reflects and perpetuates the strategic and operational divide within many health systems. But what if there was one CRM or data platform that could effectively drive healthcare growth and marketing efforts while also supporting the complex goals of loyalty and population health management?
That may sound like an ungainly Swiss Army Knife solution, but it’s actually a practical and flexible approach. The technology and data needs of fee-for-service and value-based care are more aligned and complementary than most healthcare leaders realize. With a unified data platform, a health system or physician group can deploy tools and solutions that achieve its strategic goals for volume-based care and population health. In this way, the health system can bolster its financial strength and competitive position today with commercial patients while leveraging capabilities for succeeding in risk-based arrangements at ever-growing scale.
An Innovative Way to Find, Guide, and Keep Patients for Life
Providers today face more competition for patients than ever, and those patients have growing consumer expectations for both real-world and digital service, convenience, and quality. Patients also have access to an expanding array of alternatives for primary and specialist care, spanning digital channels and telemedicine to retail clinics, ambulatory centers, corner drug stores, and even their favorite e-commerce providers (e.g., Amazon).
The Four C’s Disrupting the Market for Provider Services
ConsumerismAlready burdened with higher co-pays, today’s patients have a wider array of options for care, such as telemedicine and retail clinics, that emphasize convenience, service, and lower costs. This has helped turn patients into more discerning, more demanding consumers. |
COVID-19As it has with almost every other trend in healthcare, COVID acted as an accelerator of consumerism by steering patients away from hospitals and into the arms of telehealth, retail clinics, urgent care centers, and an ever-increasing array of alternative and satisfying options. |
CompetitionBehemoths such as CVS, Walgreens, Walmart, and Amazon have deep knowledge of consumer behavior, and are committed to changing the way primary care is delivered and experienced. Make no mistake about it: They’re taking business away from hospitals and traditional physician groups, and this siphoning will only grow. Likewise, branded surgical centers and specialty clinics are pulling acute care away from hospitals. |
ConsolidationHospital and physician group consolidation has turned local markets into regional markets and, eventually, into national markets. Those larger entities have bigger marketing budgets and an insatiable appetite for greater patient volume. |
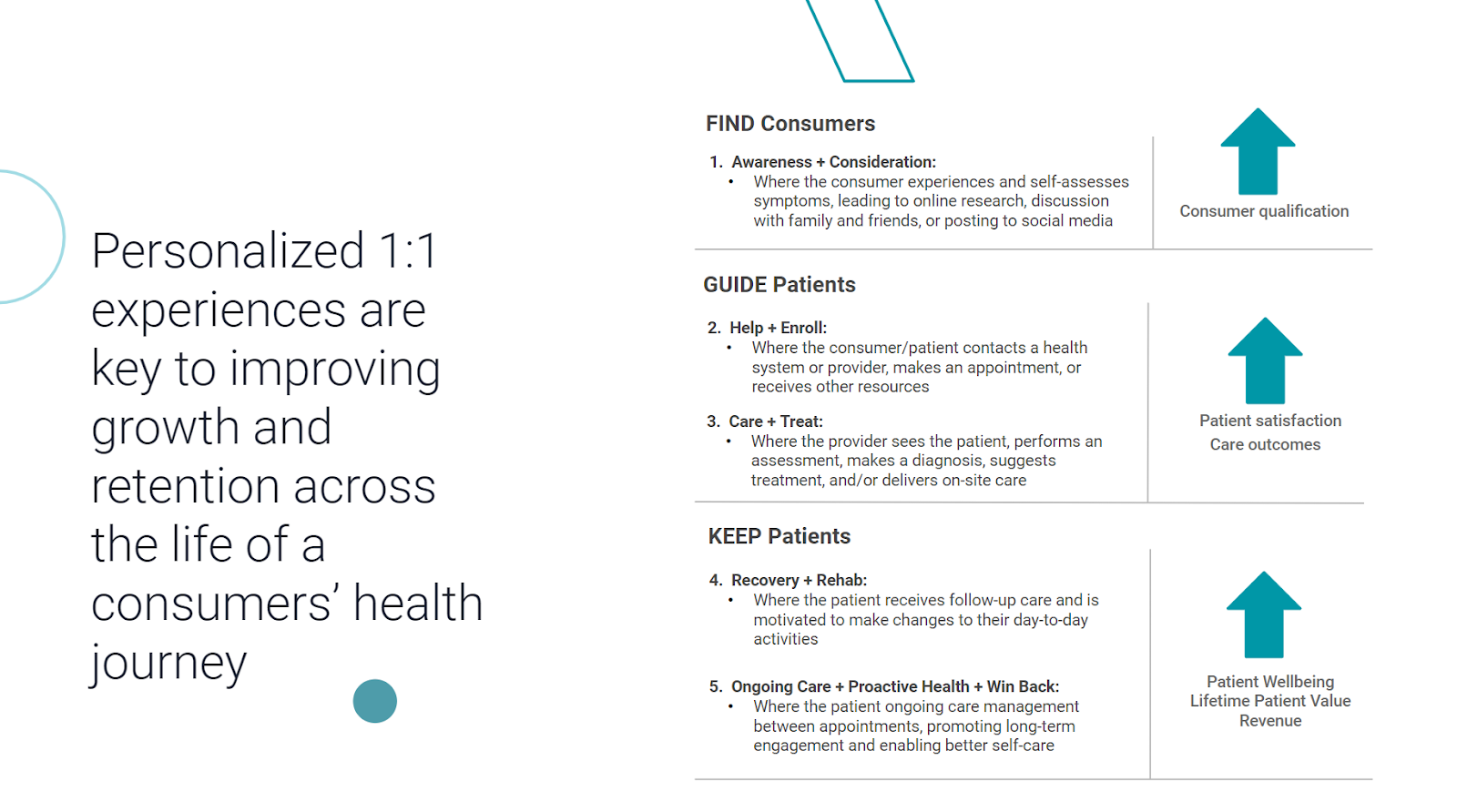
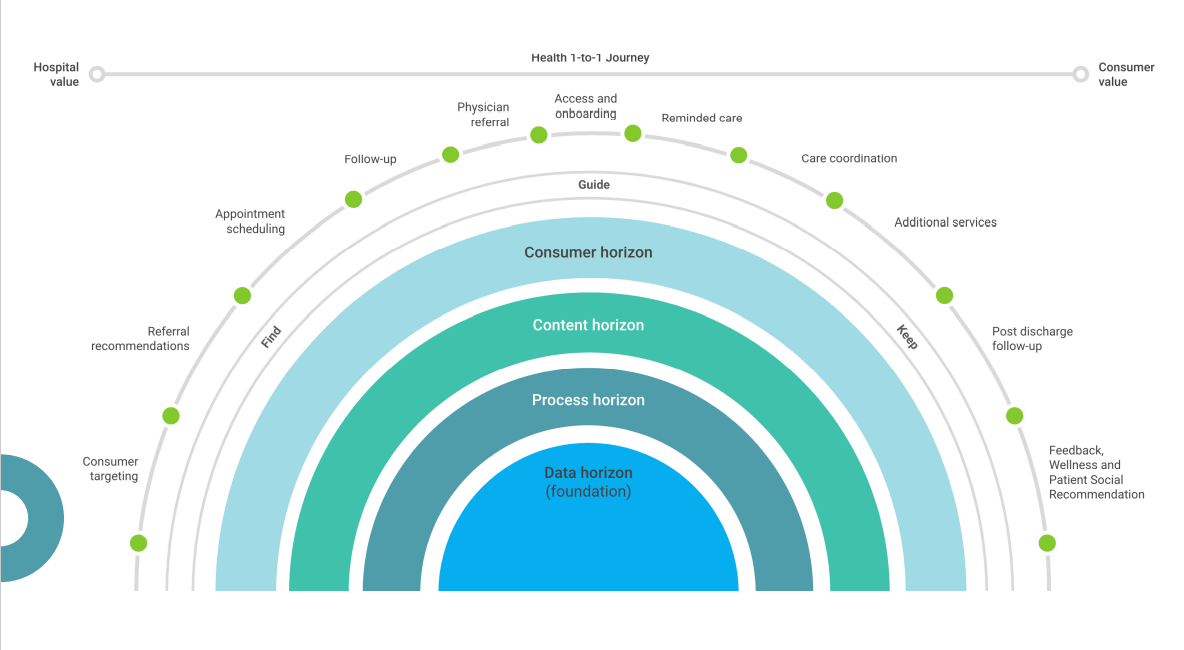
Regardless of whether they’re operating under FFS, VBC, or PHM (population health management) models, health systems and physician groups must learn how to find, guide, and keep patients in their networks better than their competitors.
Finding patients is about driving volume and growth. Guiding patients is about directing them to the right services, whether those services are designed to keep them healthy and away from the hospital or to make sure they get all the appropriate care they need in a FFS system. Keeping patients is about engaging them in their care management program or encouraging them to remain loyal to the provider the next time, and every time, they need care or have a concern about their health.
In part one of this three-part series, we focus on the challenge of Finding consumers/patients within FFS and VBC models.
Find: The Fee-for-Service Story
Traditionally, hospitals and physician groups have largely relied on patients coming to them because of illness, a health concern, or injury. Provider organizations had little reason to aggressively seek that business, but relied on billboards, ads, word-of-mouth referrals, and reputation (Best Hospitals reports, etc.) to keep their service offerings top of mind.
In today’s more competitive, consumer-driven environment, providers are turning to enterprise CRMs to help fill their pipeline of fee-for-service patients. In shifting from relatively passive to more active marketing, the new goal is to make patients feel as if they are consumers buying a service, much like they would book a hotel room, buy a plane ticket, or order prescription glasses.
In theory, many Baby Boomers and Gen X-ers still have “relationships” with primary care doctors who feed them to specialists through referrals. But today, younger patients are doing their own research online and directly seeking the services they need. This makes digital interactions the first point of contact for an increasing number of consumer-minded patients.
A CRM system will track those patients’ searches and target them with a timely stream of digital ads and offerings to entice them with promises of service, quality, convenience, and expertise. The patient self-selects by requesting an appointment, registering for an event, or visiting the clinic or ER. The CRM can then follow up with timely reminders, instructions, and referral messages.
The emphasis, in other words, is on the front-end of the care journey, with personalized connections and “white glove” treatment across multiple communication channels.
Ideally, that same CRM system would continue to track, guide, and coordinate the patient through the rest of their care journey—across every site of service, test, imaging center, referral, appointment, follow-up, payment request, etc. And ultimately, the CRM would encourage that patient to stay engaged with their doctor and loyal to the provider’s brand for future services.
The “day one” reality, however, is different. Traditional and more marketing-centric CRMs and CRM add-ons:
- Don’t provide a ready-for-healthcare contact center as a super-hub for access, triage, transitionary care, and overall experience management. Without this bridge, a consumer will never be able to receive a consistent and accurate point of entry into any health organization. They’re left to figure that out on their own.
- Don’t provide proper, regulatory-approved early care management and care coordination workflows to provide deeper, frictionless access into the heart of the health system administration, and aren’t able to adapt to consumer preferences and provide choices of where to go next.
- Don’t provide clinical data from day one. This means that, once the marketing CRM has done its job, it hands the patient over to other departments using other groups of vertical technologies that use different data and processes, which typically look and feel different from the experience the consumer/patient was just engaging with. The consumer/patient journey becomes fragmented from the start, and their experience will be inconsistent, subpar, and not satisfying—certainly nothing to rave positively about on social media.
- Don’t provide an integral physician connection that bridges the “consumer to patient to physician” transition with unified and comprehensive patient data. This time the fragmentation is even worse, because it goes a level deeper to the doctor when they open their EHR to learn about their patient. Outside the clinical record, what does the doctor know about the patient? It’s generally accepted that 80% or more of a person’s health is related to non-clinical and social drivers. But the doctor won’t have those insights in the EHR, and thus won’t be able to act on them as part of their recommendations and treatment plan. This might well be the #1 limitation of traditional CRMs and EHRs trying to enter the healthcare CRM space. They are not proficient at integrated communications and cross-departmental integration and synergy.
They also fall short in the Guide and Keep stages of a patient’s care journey. Clinical data is hard (or even impossible) for traditional CRMs to collect, sort, access, and process, partly because of the complexity of that data with its specific fields, terms, etc.; and partly because of compliance issues with protected health information and HIPAA.
Traditional vendors are trying to extend the utility of legacy retail-oriented CRM solutions through digital and physical care coordination, but to date, they haven’t had much success —just ask any provider who is using a legacy “big tech” CRM and wants to use clinical data to further personalize the care journey.
Find: The Value-Based Care Story
The same forces—consumerism, COVID, competition, and consolidation—have accelerated adoption of value-based care models and supportive technologies, though at a smaller rate and scale. Consumer-minded seniors have gravitated toward risk-based Medicare Advantage programs over traditional fee-for-service Medicare. Forty-five percent of Medicare beneficiaries are enrolled in Medicare Advantage plans in 2022, a share that is projected to rise to more than 50 percent by 2025.
CMS is also committed to moving standard Medicare increasingly to value-based alternative payment arrangements. The Shared Savings Program alone went from recruiting its first healthcare providers in 2011 to its current status as one of the largest value-based programs in the country, covering more than 11 million lives with over 525,000 participating clinicians.
A new breed of retail-savvy providers, such as UpStream Healthcare and Franciscan Health, have jumped at the opportunity to capture patients eligible for care management. And COVID has intensified efforts to address health equity gaps in under-served populations through population health services. To keep patients in VBC arrangements healthy and out of the hospital, health systems need robust data platforms that can use clinical data to better engage patients and coordinate care across multiple settings and complex payment models.
Now, at first blush, providers working with VBC models would seem to have less need to actively “Find” patients for their programs. In truth, they still need to identify the right patients within a given region or population, target those patients with messaging that encourages them to enroll or engage, and deliver a positive experience that contributes to better outcomes. In fact, because those risk pools are small, VBC models can become financially precarious if the number of attributed lives declines. Conversely, they become less risky and more profitable when the programs are scaled.
Achieving scale takes robust data, analytics, and information sharing capabilities between EHRs and other HIT and clinical systems—not to mention consumer digital devices and communication channels. The provider must be able to assess the health conditions and status of their patient population; perform the kind of risk stratification on individual patients that makes the right interventions possible and profitable; and coordinate care and social services easily across all settings, in ways that reduce administrative burdens on clinicians and provides a hyper-personalized, clinically aligned journey experience for patients.
Traditional CRMs can’t get to that n-of-1 level, and they can’t aggregate all of a patient’s data (contract status, clinical, claims, social determinant, demographic, marketing) into a unified patient record. They also typically have no way of flagging who's in an at risk contract already versus who is not. Why? At the end of the day, they don’t have the data (where’s the beef?). This effectively limits their ability to market to that patient population. Instead of knowing who that patient is in a holistic, longitudinal, and clinically personalized way (as well as retail personalized), the CRM segments the patient into a persona or group that is broad, static, and not reflective of the patient’s actual interactions with the provider organization.
Imagine how much more effective a marketing campaign would be if the CRM solution had all of a patient’s data, both as a retail consumer and as a patient with clinical requirements. Imagine how much more personalized, engaging, and satisfying that patient’s interactions with the provider organization would be if that data were accessible and readily available at every point of care and experience. Imagine what happens when a patient feels their provider “shows me they know me.”
Eliminating Barriers to Systemness
It’s been said that American health systems are systems in name only. Over the past several years, calls for “systemness” have increased with the need to optimize performance across all dimensions of a provider organization’s operations. Artificial divides between marketing, administration, clinical care, and finance impede that performance improvement.
Operating under VBC and FFS models at the same time, most provider organizations today perpetuate that divide by using different technologies and different sources of patient data and information. Today, VBC models need a unified patient record to coordinate care, enhance engagement, and achieve quality and cost containment goals. And FFS models need a unified patient record to provide the kind of “white glove” consumer experience patients increasingly expect from the moment they start to interact with the provider organization and across their entire care journey.
The notion of value-based CRM, or VBCRM for short, ensures that both operational models benefit in terms of financial performance, outcomes, and experience by bringing traditional CRM and contemporary PHM data together in a longitudinal patient record—creating a holistic, single source of marketing truth about the patient. Bridging these worlds also better prepares organizations to actually take on more risk over time. That is true healthcare marketing, where the emphasis is truly on delivering quality healthcare and experiences at every step of a consumer-to-patient journey.
Lastly, embracing this approach—bridging the FFS and VBC worlds with a healthcare CRM that understands and leverages population health data in both contexts—better prepares organizations to take on more risk over time, which is the inevitable end state of US healthcare. And in the end, the patient benefits most of all.
As Innovaccer’s chief medical officer, Dr. David Nace, puts it: “The antidote to healthcare fragmentation is systemness, which is alignment across finance, clinical care, and culture. But that requires a platform that’s pulling data from every source, including every care setting and every contract.”
The question shouldn’t be, “What’s the best CRM for FFS and the best data platform for population health?” The question should be, “What’s the best solution for healthcare?” That question now has an answer: VBCRM.
How Can Innovaccer Help?
The Innovaccer platform’s Enterprise Customer Relationship Management (CRM) solution uses a unified patient record to boost patient acquisition, enable clinically personalized patient journeys, enhance retention, and improve the bottom line.
By integrating and activating all patient data through a longitudinal consumer/patient record, health systems can attract new consumers more effectively; accurately guide patients throughout their care journey; and better coordinate episodes to improve experiences, care, and your organization’s financial outcomes.
As the industry’s only Enterprise CRM built from the ground up exclusively for healthcare—populated with all of your relevant CRM, EHR, HIT, consumer, and patient data from day one—there’s simply nothing else like it in healthcare … and no faster way to get started accelerating your success with consumer and patient engagement.
About Innovaccer
Innovaccer Inc. is the #1 data platform for value-based care. The Innovaccer platform unifies patient data across systems and care settings, and empowers healthcare organizations with scalable, modern applications that improve clinical, financial, operational, and experiential outcomes. Innovaccer’s EHR-agnostic solutions have been deployed across more than 1,600 hospitals and clinics in the US, enabling care delivery transformation for more than 96,000 clinicians, and helping providers work collaboratively with payers and life sciences companies. Innovaccer has helped its customers unify health records for more than 54 million people and generate over $1 billion in cumulative cost savings. The Innovaccer platform is the #1 rated Best-in-KLAS data and analytics platform by KLAS, and the #1 rated population health technology platform by Black Book. For more information, please visit innovaccer.com.
See the industry’s most advanced decision support system