VBCRM Part II: Caring for Patients like Human Beings, Not Contracts

A value-based CRM brings CRM, pop health, and digital-experience data, insights, and workflows together—independent of payment models, including FFS—to guide patients through the clinically personalized, continuous care journeys they want today
The schism between fee-for-service and value-based care business models presents a false choice over technology systems to healthcare leaders, blocking them from delivering truly personalized 1:1 health experiences to patients throughout their care journey. The question shouldn’t be, “which system do I need for FFS and which do I need for population health or value-based care?” The question should be, “which system do I need to enhance the experience, health, and loyalty of consumers?”
Health systems spent $14 billion globally on CRM technology in 2021, 50% of that in the US. That’s expected to grow at a CAGR of 8.4% from 2022 to 2030. And yet, despite that massive investment and lofty industry-wide strategies for meeting healthcare consumerism head on, satisfaction with the “experience” of U.S. healthcare is tepid at best.
Ask yourself if you’ve ever heard someone express delight over a healthcare encounter. Ask yourself how loyal you think patients are to any particular health system. Ask yourself if your organization’s CRM strategy makes a meaningful difference in service, health outcomes, care coordination, brand strength, market share, or people’s lives. I’ll wager your CRM falls short on these basic functions, and that you put a lot more effort into “making your EHR work” relative to the value it provides your organization in return.
Competing Definitions: The Old and the New
In the era of healthcare consumerism, we need a new definition of CRM if we are to realize its full, as-yet untapped potential.
Traditional CRM (as defined by HIMSS):“... an organization-wide strategy for managing an organization’s interactions with its patients and their supporting infrastructure, suppliers, providers, and/or employees using CRM technologies. It seeks to optimize the way we establish and nurture meaningful and sustainable relationships in efforts to enhance patient experience, improve population health, reduce costs, and improve the work life of healthcare providers – ultimately leading to increased trust in and loyalty to the organization”. |
Value-based CRM:VBCRM is far more than a marketing function. It’s an enterprise healthcare communications platform, independent of reimbursement models, that spans and integrates the entire clinical patient journey, from finding new consumers/patients to guiding them through every step of their care, and keeping them retained for life. |
As I covered in the first article in this series (VBCRM: Bridging Healthcare’s Greatest Divide), a lack of “systemness” is at the root of this problem, exacerbated by the technological divide inherent in different IT platforms. In part one, I talked about how improving a hospital’s systemness by unifying consumer behavior and population health data can have a transformative impact on finding and acquiring new patients, regardless of the reimbursement model in use, be that FFS, VBC, or some other APM.
Now I am going to talk about how systemness (or the lack thereof) impacts the work of guiding patients through their care experience. And in my next and final piece in this series, I’ll describe the power this has on keeping patients loyal for life.
Healthcare Needs a GPS for Guiding Patient Care
When it comes to guiding patients through their care journey, deploying an enterprise CRM for FFS customers and a pop health data platform for those under shared- or full-risk models creates barriers to systemness that make both solutions less effective. By unifying consumer CRM and patient population health data through a single longitudinal record, providers remove the artificial barriers that exist between marketing, administration, clinical care, and finance, improving performance across all of these areas.
Examining how patients can be supported in navigating their healthcare journey illustrates the power of unified patient health data. Fee-for-service entities can benefit from infusing web and CRM personalization with population health data, analytics, and insights; while risk-bearing entities can expand and tune their risk pool, improve care journeys, keep patients in-network, and enhance care quality by leveraging pop health data with retail “CRMesque” communication programs.
Let’s see how that works.
Guiding patients is all about having the right data and the right message, so you can deliver the right care to the right person at the right time, all the time—whether that’s to keep them healthy and away from the hospital under a value-based or alternative payment model, or to make sure they get all the care they need in a fee-for-service system, only when they need it.
For value-based care, a population health platform that unifies patient data and insights across EHRs, HIT systems, and care settings—while integrating with and supplementing legacy or archaic EHR clinical workflows—is essential if the health system wants to avoid hemorrhaging money on those contracts. Giving care teams a single source of patient truth at the point of care across an entire journey, including visibility into social determinants that impact local community interactions and health equity, enables them to effectively engage patients, coordinate care, change behaviors, and improve outcomes in a way an EHR can’t do on its own.
But how in the world does that kind of technology investment make sense with fee-for-service patients? If healthcare has an implicit bias about traditional, fee-for-service care delivery, it’s that “service” is at best secondary and at worst antithetical to clinical expertise. This is reinforced by the fact that providers are paid regardless of outcomes and patient experience.
In a competitive healthcare marketplace, however, a health system that fails to meet consumer expectations for smooth and seamless care coordination, personalized engagement (“show me you know me”), convenient real-world and digital services, and high-quality outcomes and experiences will inevitably lose its fee-for-service patients to providers who do a better job at the “service” part.
Many digital officers are now steadfastly equating this phenomenon to moments such as buying a latte from Starbucks or even booking an appointment for a haircut. A consumer is going to wonder why their small business hairstylist does a better job of reminding them about an upcoming appointment than their big business health system.
“Why?” indeed. Consumers don’t know or care how the health system is being reimbursed. All they know, remember, and talk (or post) about with friends and family is what their experiences were like and the outcomes they’re living with.There’s more PHI on Facebook than in every health system in America. And consumers are sharing the good and the bad stories with their online and real-world social networks.
Individually, CRMs and EHRs simply can’t approach that required level of insight, engagement, and workflow integration. And in their defense, they were never designed to. They rely on multiple, fragmented sources of patient truth. Conversely, a single platform that can engage and coordinate care for all patients, regardless of the payment mechanism, can help a health system achieve its strategic and financial goals in each business model, through a single source of patient truth.
To paraphrase Superman, this looks like a job for VBCRM. It puts an end to the false choice of “we need a CRM for our FFS business, and a pop health platform for our risk-bearing businesses.” In fact, you need a healthcare CRM that bridges the schism and brings both worlds together, to achieve 360° of patient engagement that's not possible otherwise or anywhere else.
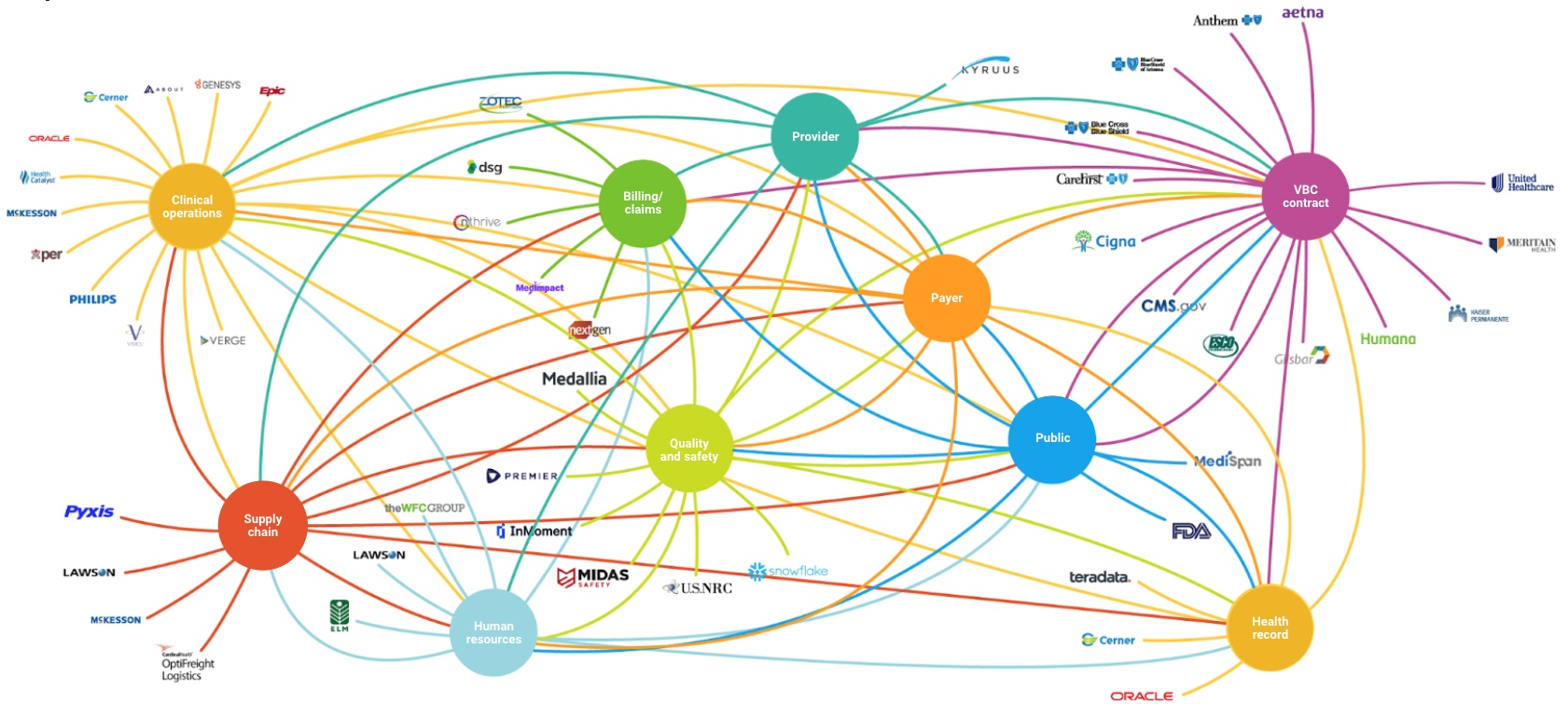
Fig. 1: The typical health system IT infrastructure makes it impossible to harness the full value of data, analytics, insights, and workflows for effective VBCRM
Guide: The Value-Based Care Story
Whether through ACO REACH, Managed Medicaid, Direct Contracting, an employer agreement, or even traditional Medicare with quality metrics in play, a health system can find itself in a complicated array of contractual arrangements that include some level of risk for different patient populations. From the outset, that presents challenges.
“Finding” patients is hard. Lists can be out of date and inaccurate. Patients may not know they belong in one program or another. Lacking comprehensive data, the health system can struggle to identify the right patients and establish contact with them. This is especially true for Medicaid beneficiaries who might have no fixed address or permanent phone number.
Once those patients are enrolled, however, the real work begins. In short order, the health system needs to assign each patient a risk score. Are they behind on testing or assessments? Do they need to be enrolled in a care management program? Do they have the proclivity to develop a more serious and costly condition? Payment is based on level of acuity, so it’s critical to develop an accurate, comprehensive understanding of each patient’s current health status and future needs. In other words, you need to build a tight 1:1 relationship.
By pulling rich data from different sources, the health system can create a high-definition portrait of each patient, and much faster than it could through isolated care encounters. This helps the health system design a customized set of interventions—from regular wellness visits to full-blown care management programs—tailored to the patient’s risk profile, while continuing to stay connected, track statuses, coordinate care, and support care teams at the same time.
And that last part is the critical connection to get to an “experience.” These technical moments need to happen in unison at the same time. Data must be quickly connected and rationalized in nano-seconds, assimilated into the proper unified workflow (also in nano-seconds) and then presented in the simplest way humanly possible in (you guessed it) nano-seconds.
Ultimately, to be successful in population health and value-based arrangements, a health system also needs to be able to change patient behavior. And behavior doesn’t change quickly, if at all, when the path to get there is riddled with roadblocks, miscommunication, no communication, and uncommon language that some people went to medical school for years to learn. The health system can’t be passive about expecting patients to keep appointments, get blood work done, adhere to medicines, adopt healthy lifestyles, manage depression, reduce blood sugar levels, and go to urgent care instead of the emergency department.
That takes ceaseless patient engagement rooted in ease and comprehensibility, backed by an integrated technology and data platform that doesn’t diminish the high level of understanding required. Moreover, a parallel system of support is needed for the provider network. On their own, clinicians can’t be expected to follow the stipulations of multiple contracts for multiple patients when they’re prescribing medicines, making referrals, scheduling tests, or recording clinical data.
And in a growing population routinely branched and forked by technology at almost every level, they can’t be expected to “know” each patient well enough to engage them effectively on their health over time. The workflow around the guided patient journey in VBC must be supported by intelligent and automated data with the right prompts, signals, insights, and information reaching the care team and the patient at the point of care at the moment it’s requested.
And it must be integrated into their existing EHR clinical workflow or, as the CIO of a major health system recently told me, “they simply won’t use it.” Being able to change physician and clinician behavior is equally important and directly proportional to the success of those to whom providers serve every single day.
Guide: The Fee-For-Service Story
On the fee-for-service side, what happens after a consumer looking for healthcare services becomes a patient? Once that consumer has made an appointment, walked into the emergency department or urgent care, followed through on a referral, or been scheduled for a procedure, they are “in the system.” Typically, however, there’s nothing systematic about that experience going forward. For too many patients, the journey—whether it lasts a few visits or a few years—feels bureaucratic, impersonal, uncaring, and marked by transitions that are rarely automatic or seamless.
In the guide stage of fee-for-service, health systems rely almost entirely on their EHRs to communicate with patients and coordinate across care teams, to the detriment of all. Messages, prompts, and follow-up information should be automatic and personal, but they’re not. Interactions lack continuity, appropriate urgency, or any sense of responsiveness to the patient’s needs and circumstances. To put it plainly, the EHR is not and will never be a relationship management tool. It’s not in EHR vendors’ DNA to depart from a business model they’ve maintained for over 40 years; that is, the claim system of record. They’re cut from an entirely different IT cloth, and have little to no understanding of day-to-day human behavior or consumers’ decision making process from a psychological and physiological point of view.
Imagine a different FFS world in which patient communication was always timely, personal, and on the mark—one in which, leading up to a surgery, intervention, or test, the patient received appropriate and helpful reminders designed only for them. In this model, the day before an appointment, the patient is sent a map of where they are to go, with step-by-step instructions, and introductions to the care team waiting for them. Then, post-procedure or post-visit, the patient receives follow-up information and check-ins about status, experience, or progress, as well as clear details about billing and a simple way to pay. And again, these communications are only for them.
Imagine if all communications were calibrated to perfectly suit the patient’s unique circumstances, digital behavior, thought process, and condition—including their emotional, intellectual, physical, and financial capacity to process and follow through. Imagine, too, that on the other side of that intervention or visit, the care team and administrators were similarly informed and supported automatically and intelligently through their workflow. Imagine that the hospitals, physician clinics, specialist offices, ambulatory care clinics, urgent care clinics, rehab centers, testing and imaging sites, marketing departments, finance departments, and pharmacies were also included in that web of connections.
Imagine that all of the patient’s data helped make their care and experience better not just for one intervention, but for all encounters with the health system for years to come—and again, not just limited to the patients, but including those within the health system’s web of connections. If one link in the guided journey is broken for any one party, then it's broken for all. Those who talk about "patient engagement" without mentioning "physician engagement" and engagement across the guided journey’s full web of connections don't understand, and can’t support, a truly holistic guided care journey.
Wouldn’t a patient, in such a well-guided and interconnected system, be more likely to return for repeat business if all of these scenarios weren’t imaginary? Wouldn’t a physician or call center triage nurse feel more empowered, supported, and engaged? Given the relative size of their fee-for-service book of business and the likelihood that competition for market share will only intensify going forward, shouldn’t every health system be hungry for that level of systemness?
While the EHR itself isn’t capable of supporting this depth of guided care for patients and their caregivers, the technology to do so, which leverages the EHR’s data and more to usher in the systemness required, is here today. In FFS as in VBC or any APM, it’s all about having the right data and delivering the right message, so you can provide the right care to the right person at the right time, all the time.

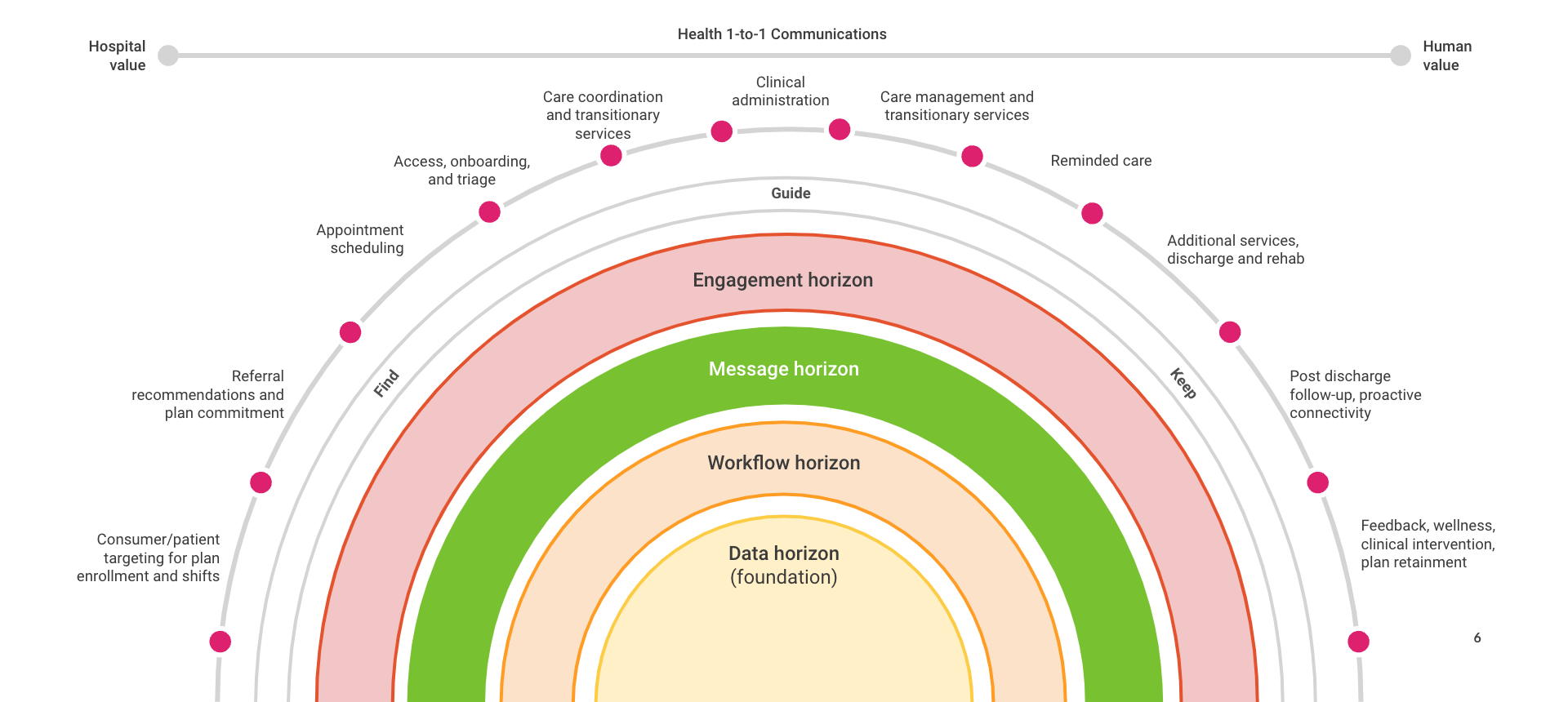
Fig. 2: Guiding clinically personalized 1:1 experiences for a better care journey and improved outcomes
Integrating the Data, Expanding the Aperture
Achieving systemness is impossible with traditional siloed technology systems such as EHRs or legacy CRMs. It’s also impossible when the health system deploys one technology solution for its FFS patients and a different one for its at-risk patients.This is the false choice that the schism between FFS and value-based models offers us.
When platforms are routinely branched and forked, any increase in data volume or number of data streams won’t make healthcare delivery easier. It will make it more complex and error prone. Indeed, we’re already there. At most any health system today, when Mrs. Smith visits the ED for heart palpitations, the nurse or doctor who sees her won’t know this is the same Mrs. Smith enrolled in a diabetes care management program who’s missed multiple appointments to get her blood work done.
Effectively, she’s two (or more) different people every time she interacts with the different systems. And, Mrs. Smith’s clinicians also won’t have the energy, time, or motivation to practice different kinds of medicine depending on the current claims model at play. They just want to provide Mrs. Smith with appropriate care and follow-up regardless of how she’s engaging with the system.
When a health system brings all of its patient data together (can I say “gets its act together?”) in a systematic way, it opens its aperture to a wider volume of patients, yet can treat each and every patient like a human being in need, regardless of coverage or where they are on their care journey. And as we’ll see in my next article, a VBCRM approach can also support and inform the health system’s most critical strategic goal: Keeping patients loyal for life.
How Can Innovaccer Help?
The Innovaccer platform’s Enterprise Customer Relationship Management (CRM) solution uses a unified patient record to boost patient acquisition, enable clinically personalized patient journeys, enhance retention, and improve the bottom line.
By integrating and activatingall patient data through a longitudinal consumer/patient record, health systems can attract new consumers more effectively; accurately guide patients throughout their care journey; and better coordinate episodes to improve experiences, care, and your organization’s financial outcomes.
As the industry’s only Enterprise CRM built from the ground up exclusively for healthcare—populated with all of your relevant CRM, EHR, HIT, consumer, and patient data from day one—there’s simply nothing else like it in healthcare … and no faster way to get started accelerating your success with consumer and patient engagement.
About Innovaccer
Innovaccer Inc. is the data platform that accelerates innovation. The Innovaccer platform unifies patient data across systems and care settings, and empowers healthcare organizations with scalable, modern applications that improve clinical, financial, operational, and experiential outcomes. Innovaccer’s EHR-agnostic solutions have been deployed across more than 1,600 hospitals and clinics in the US, enabling care delivery transformation for more than 96,000 clinicians, and helping providers work collaboratively with payers and life sciences companies. Innovaccer has helped its customers unify health records for more than 54 million people and generate over $1 billion in cumulative cost savings. The Innovaccer platform is the #1 rated Best-in-KLAS data and analytics platform by KLAS, and the #1 rated population health technology platform by Black Book. For more information, please visit innovaccer.com.

