
CMS Just Made Your Post-Acute Strategy a Financial Line Item



The FY 2027 IPPS rule makes episode-based payment mandatory at national scale. Seven years of data already show who wins and who pays back. The difference isn't clinical. It's infrastructure.
The Bigger Story Inside the FY 2027 Rule
The FY 2027 IPPS Proposed Rule dropped April 10, 2026. The headline number is a 2.4% net rate increase, about $1.9 billion in total hospital payments. Important, but not the part that should be keeping CFOs up at night.
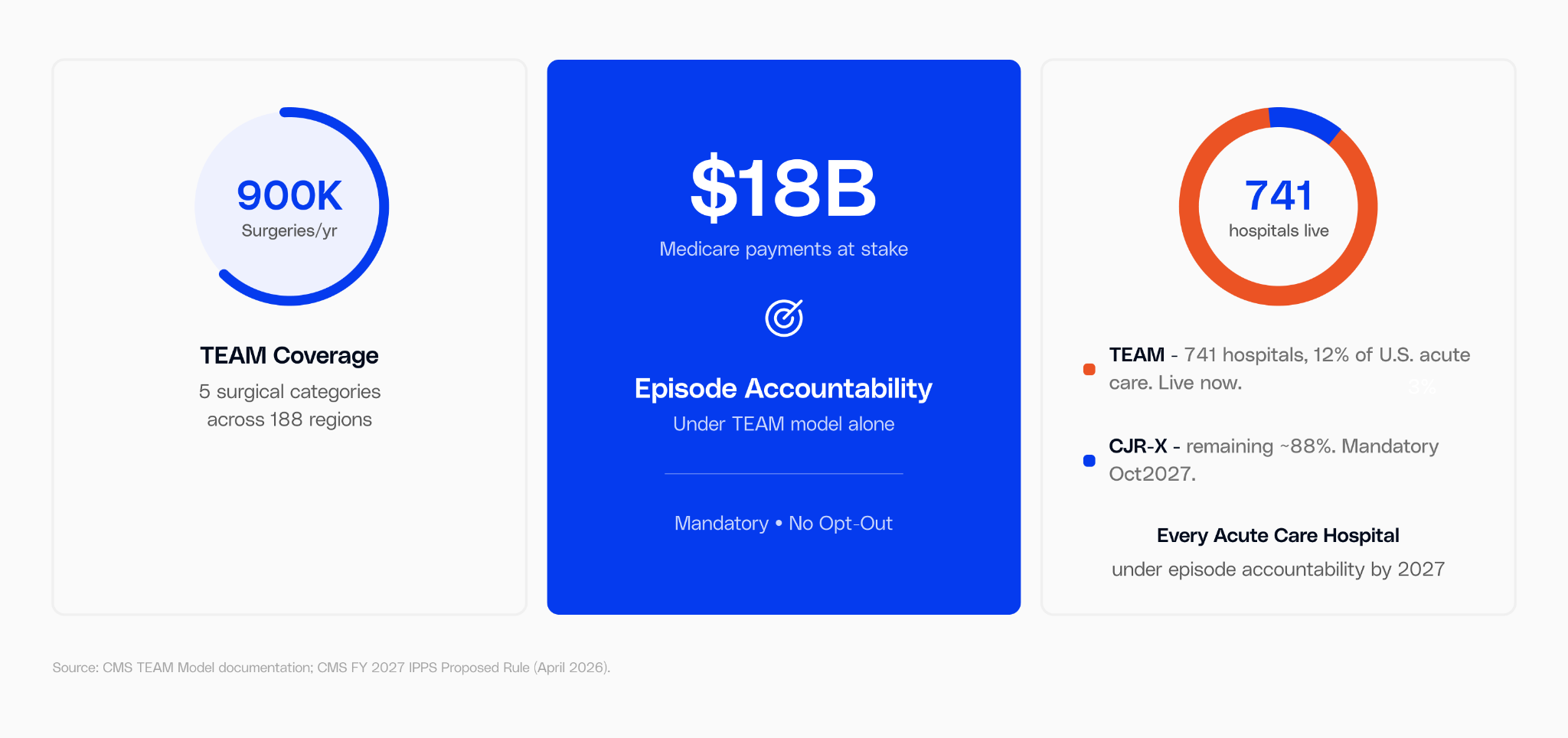
The bigger story: two mandatory payment models that change how hospitals get paid for surgery. Not "voluntary." Not "demonstration." Mandatory. One is already running. The other kicks in 18 months from now. And we already have seven years of data showing who wins under this kind of model and who writes a check back to Medicare.
The difference wasn't surgical quality. It was whether the hospital could see what happened after the patient went home.
Why This Is Different
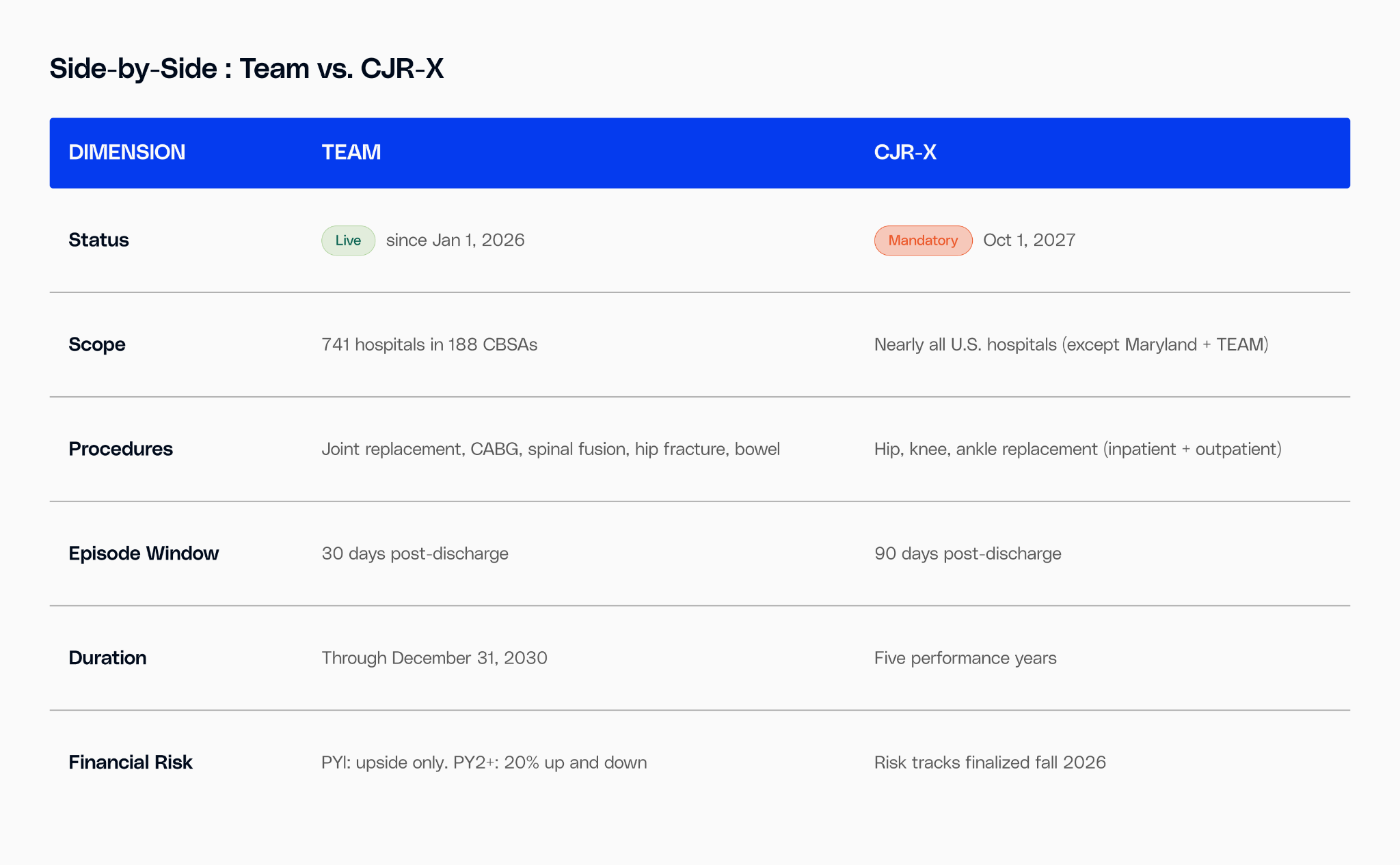
CMS calls CJR-X the first mandatory, nationwide test of episode-based payment.
This is not a voluntary demonstration. Under TEAM and CJR-X, virtually every acute care hospital in the country becomes accountable for what happens after the patient leaves the building. The quality measures are tightening in the same direction: new measures for FY 2029-2030 cover post-surgical blood clots, advance care planning, malnutrition, and excess hospital days after diabetes care.
Episode Economics
Follow the Money: 45% of Your Episode Cost Is Post-Discharge
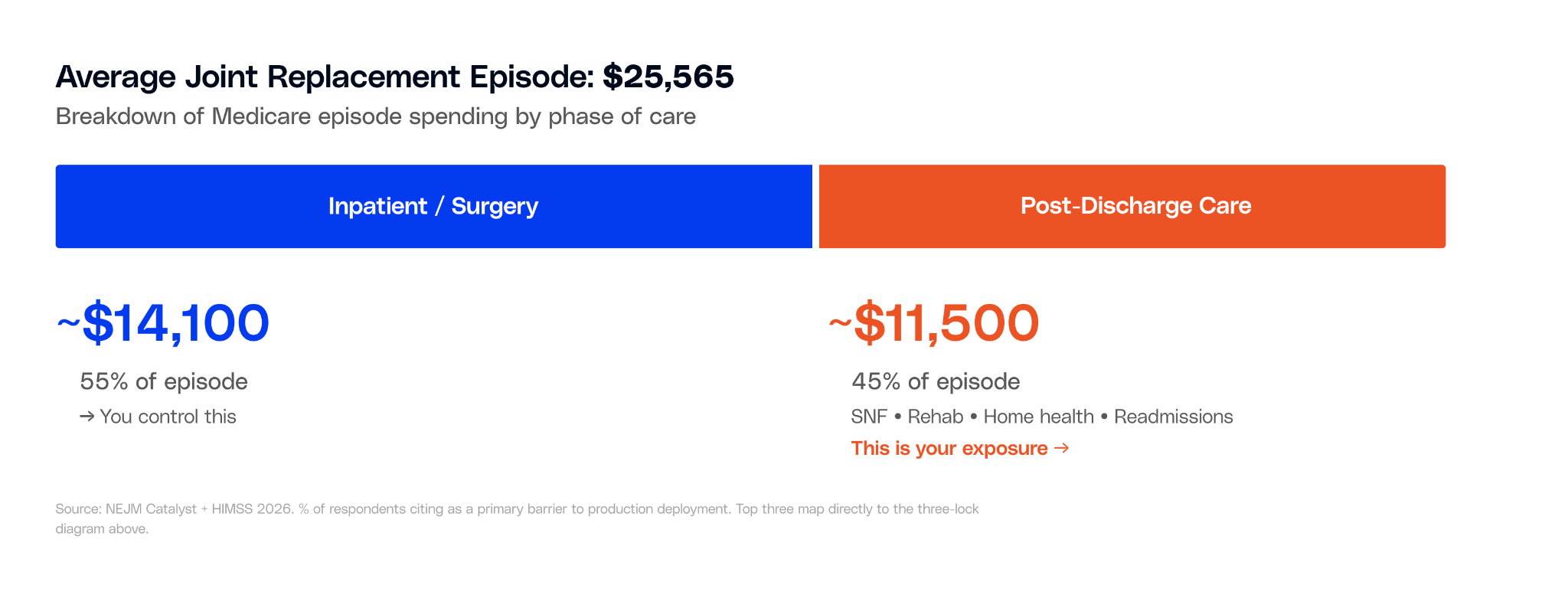
A typical Medicare joint replacement episode costs $25,565 on average. About 55% covers the surgery and hospital stay. The remaining 45%, roughly $11,500, goes to what happens after: skilled nursing facilities, inpatient rehab, home health visits, follow-up appointments, and any readmissions.
Under TEAM and CJR-X, your hospital is financially responsible for both sides. And the data from the original CJR model shows that nearly all the cost savings came from the post-discharge side, not the surgical side.
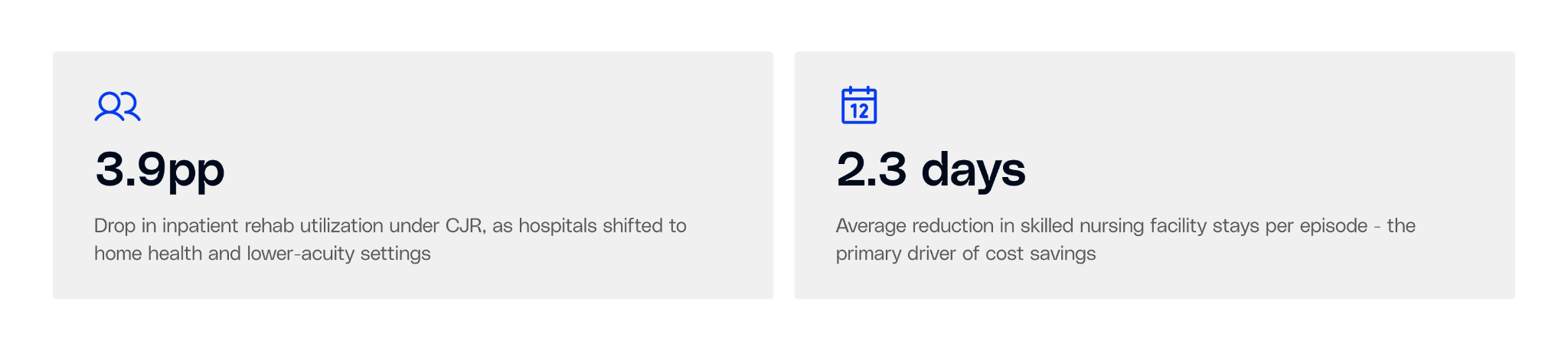
Hospitals that saved money under CJR didn't change their surgical technique. They changed their discharge patterns: fewer patients sent to inpatient rehab (down 3.9 percentage points), shorter SNF stays (2.3 fewer days), and more patients going directly home with home health support.
Seven Years of Data
Who Won, Who Lost, and Why
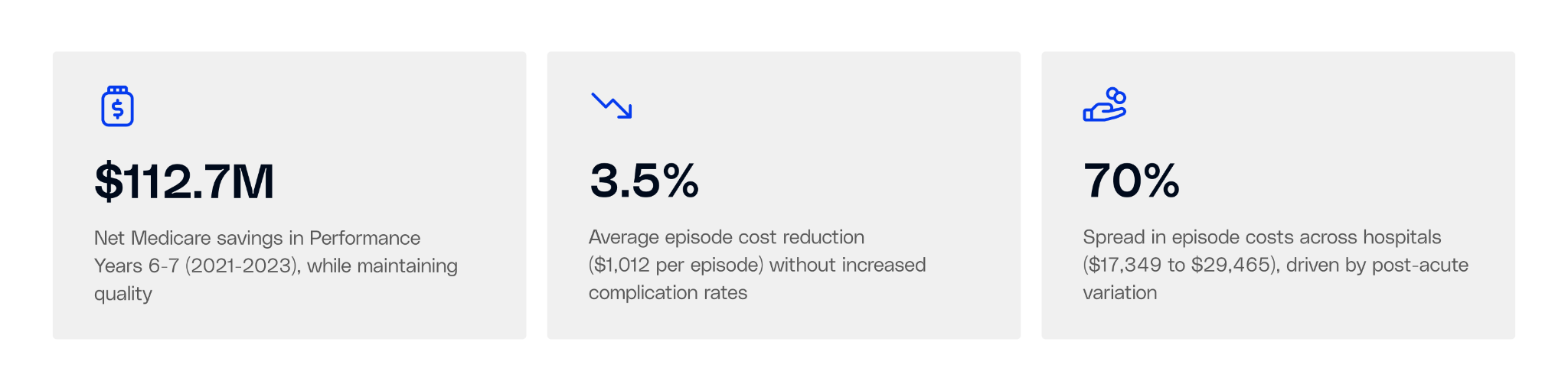
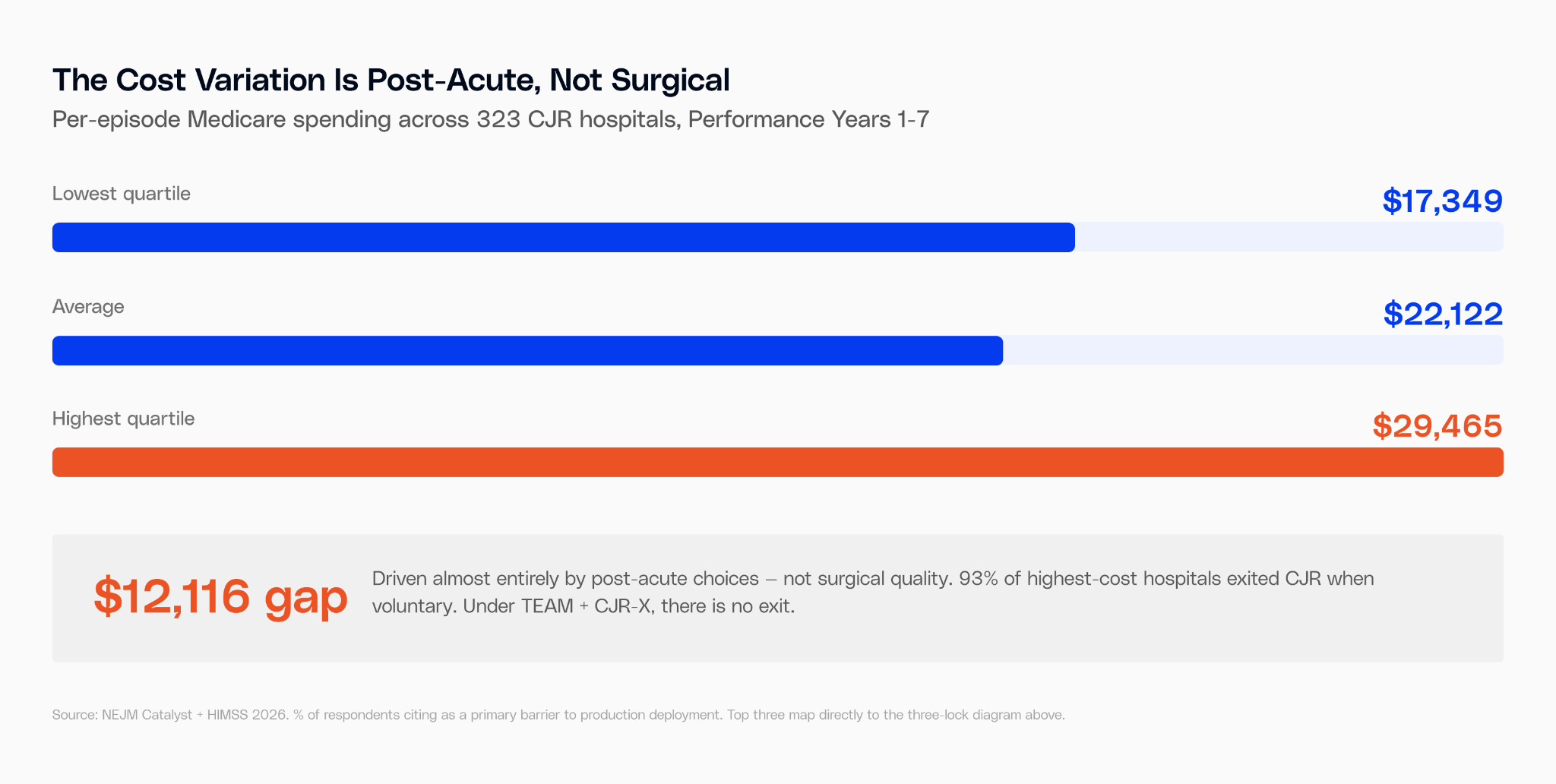
The original CJR model ran from 2016 through 2023. 323 hospitals. 98,000+ patients. Seven performance years. CMS published all of it. The data tells a clear story about where performance separated.
The Infrastructure Gap, Visualized
CJR performance split along a clear line: hospitals with coordinated post-acute networks earned money. Those without them paid back to Medicare. Safety-net hospitals were disproportionately penalized.
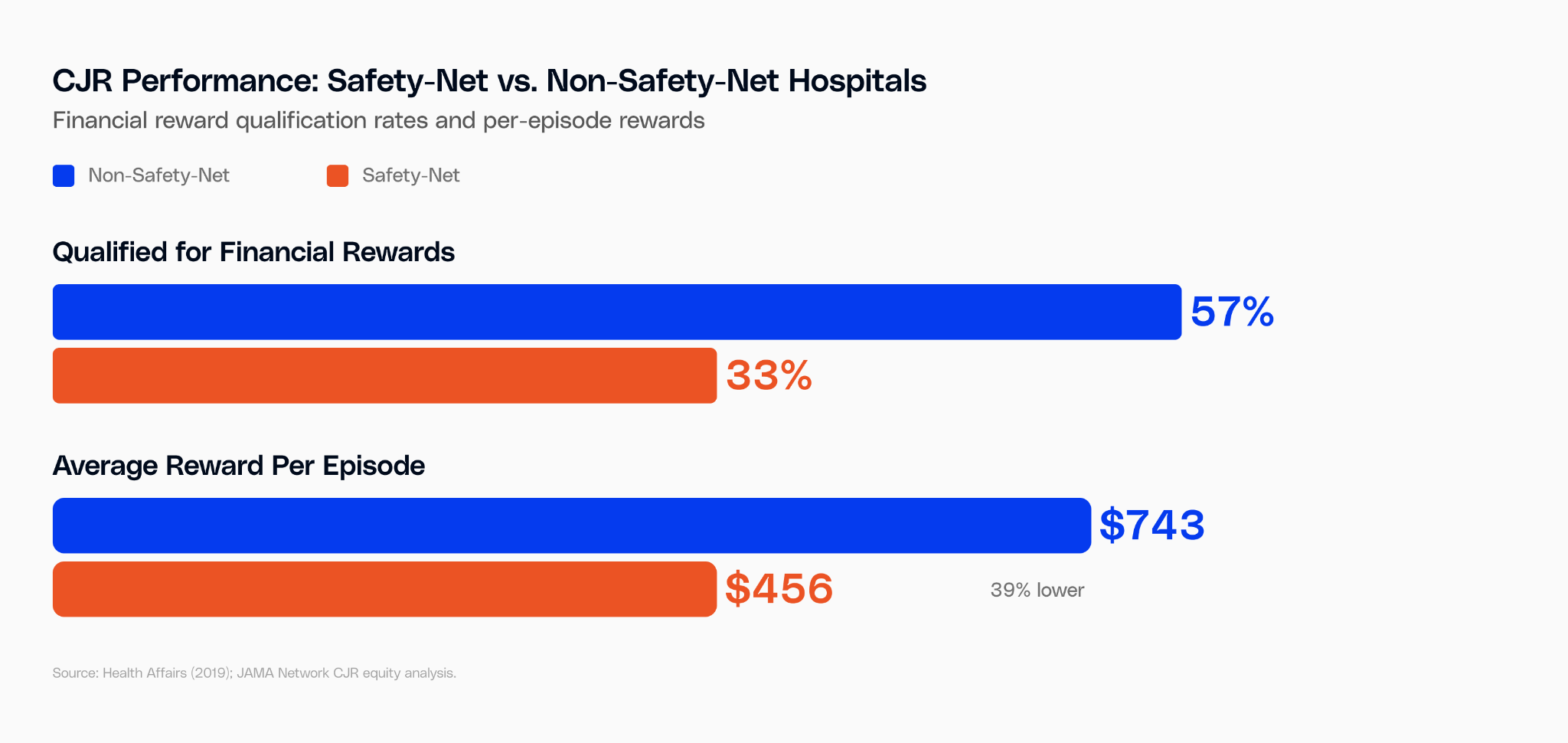
Safety-net hospitals weren't performing worse surgeries. They had weaker post-acute networks, more fragmented referral relationships, and less data on what happened after discharge. By 2019, 87.9% of safety-net hospitals were in penalty territory. The model penalized the infrastructure gap, not the clinical gap.
TEAM includes new equity provisions: mandatory social needs screening, risk-adjusted benchmarks, and lower-risk tracks for hospitals serving underserved communities. But the underlying dynamic hasn't changed. Your reconciliation payment reflects your post-acute data, or the absence of it.
The Structural Argument
The gap between winning and losing hospitals was never clinical. It was infrastructure.
CMS published seven years of data showing exactly what separates the hospitals that earn money from those that pay it back. The answer was post-acute coordination, discharge visibility, and the ability to see the full episode in a single data layer.
That's not a future problem to plan for. It's the financial exposure that's already running under TEAM, and that becomes national under CJR-X in 18 months.
Readiness
Can You See the Full Episode?
The average hospital works with 37 skilled nursing facilities and 23 home health agencies. Working with them isn't the same as coordinating with them.

The Timeline
- Now through June 9, 2026 Comment period closes
Your window to influence the final rule. CJR-X risk track details and target pricing finalized in the fall.
- Q3 2026 — TEAM PY1 data accumulates
TEAM hospitals are in upside-only Track 1 through 2026. But PY1 performance sets baselines for when downside risk activates in 2027.
- Fall 2026 — Final CJR-X rule published
Target prices, quality thresholds, and risk tracks become definitive. Hospitals will know their exact financial exposure.
- January 2027 — TEAM moves to downside risk
Most hospitals shift to Track 3: 20% upside and downside. Every dollar over target price is a reconciliation line item.
- October 1, 2027 — CJR-X goes live nationally
90-day episode accountability for hip, knee, and ankle replacements at virtually every hospital in the country.
The Operational Reality
The Problem With Doing This Manually
For every episode-eligible patient, someone on your team needs to identify them before discharge, match them to the right post-acute facility, coordinate the authorization, track their recovery for 30 to 90 days, follow up if they're trending toward a readmission, and reconcile costs against target prices. Then do it again. And again.
A busy hospital runs 500 to 1,000+ episode-eligible surgeries a year. Each one requires multiple touchpoints across settings your EHR doesn't see. Care transition coordinators currently spend 2 to 4 hours per patient on this work — phone calls to SNFs, prior authorization paperwork, discharge documentation, readmission tracking.
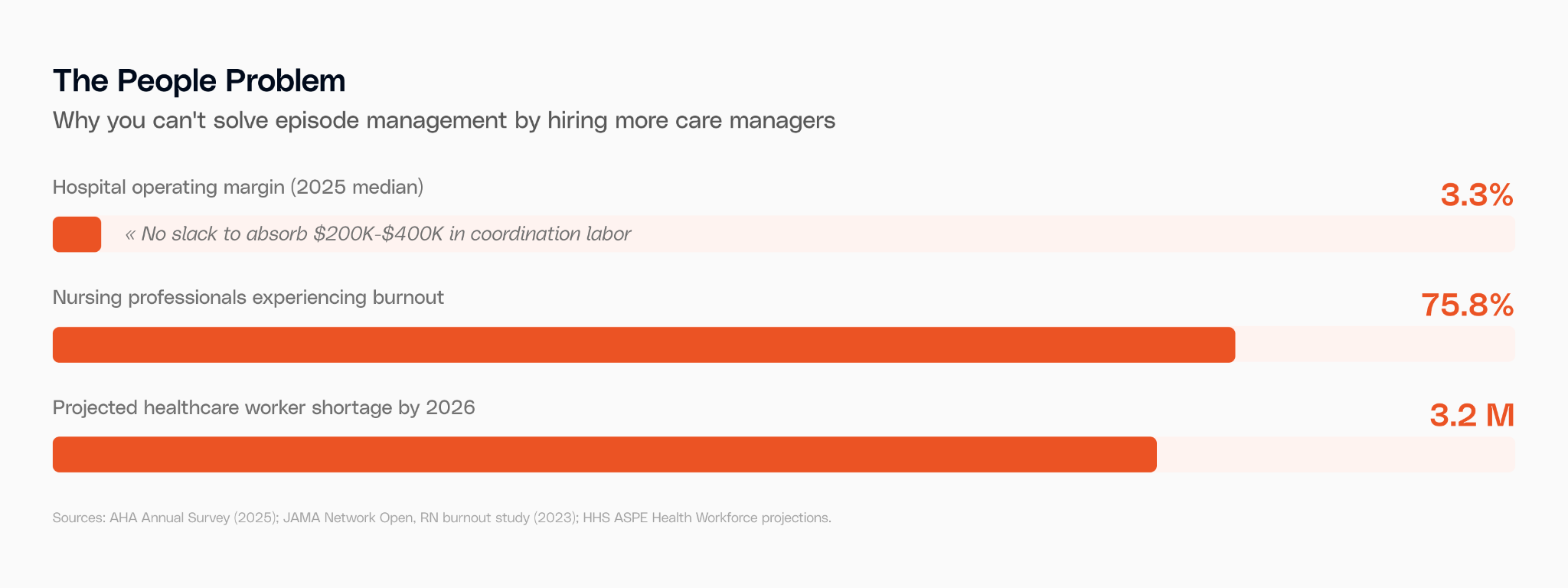
A dedicated RN care manager costs about $99,000 a year. A 500-episode program needs 2 to 4 of them just for episode coordination. That's $200K to $400K in labor before you've touched technology, reporting, or reconciliation. On a 3.3% margin, most hospitals don't have that slack. And when these positions go unfilled, the work falls to floor nurses already managing 9+ patients per shift.
The Lesson From BPCI-A
BPCI-A, the voluntary predecessor to TEAM, is the closest comparison we have.

"Many organizations are not of adequate size or in a financial position to support the investments necessary to transition to mandatory bundled payment models." American Hospital Association, response to TEAM rollout
The difference this time: there's no opting out. Which means the path forward isn't "hire more care managers." It's redesigning how the work gets done.
The Path Forward
How Do You Manage 1,000 Episodes Without Burning Out Your Team?
Episode-based payment models don't fail because hospitals provide bad care. They fail because the data is fragmented and the work of connecting it falls on people who are already at capacity.
Your EHR sees the admission and the discharge. It doesn't see the 90 days that follow. The SNF has its own system. The home health agency has another. The readmission shows up weeks later, and by then the reconciliation damage is done.
Innovaccer's platform, Gravity, the Healthcare Autonomy Platform, connects the full episode: clinical, claims, and post-acute data unified into a single layer. But the data layer alone isn't enough. What makes the difference is what sits on top of it: AI agents that handle the operational work that today consumes your care team's time.
Your team stays at the center. Agents handle the chase work, surface the signal, send the packet, flag the risk. Your care managers make the calls that actually matter.

We've seen this across dozens of health systems. The ones that capture the upside under bundled payment models have coordinated data and automated workflows. The ones that absorb the downside are doing the same work manually, with staff they can't keep or can't hire.
CMS has published seven years of evidence showing what the gap costs. TEAM is live. CJR-X is 18 months out.
The Bottom Line
This rule doesn't change what good care looks like. It changes who gets paid for delivering it.
The hospitals that start building now, the data infrastructure, the PAC partnerships, the transition workflows, will own the upside. The ones that wait will spend 2028 explaining the variance to their boards. This isn't a policy update. It's a deadline.
If you want to know more, talk to an expert.

with the Power of Comet
.svg)
.svg)

.svg)

