Two new CMS payment models take effect in 2026 and 2027. Both tie reimbursement to clinical outcomes rather than volume. Both require technology infrastructure that most health systems have not built. And both reduce payments after Year 1, which means the organizations that delay a platform decision will face the steepest implementation costs precisely when their margins tighten.
The CMS ACCESS model, launching July 2026, pays $15 to $35 PMPM for chronic care management across four clinical tracks, with 50% of that payment contingent on hitting defined clinical improvement targets. The LEAD model, replacing ACO REACH in January 2027, introduces a 10-year fixed benchmark with no rebasing. Together, they represent CMS's clearest signal yet: technology-enabled, outcome-accountable care delivery is the baseline expectation for the next decade of Medicare.
This is the context in which your population health management platform decision now sits. The feature checklists that guided PHM vendor selection three years ago no longer capture what matters. The question in 2026 is whether your platform can activate data into governed workflows, support the specific reporting and interoperability requirements of ACCESS and LEAD, and deliver AI-driven care orchestration at production scale rather than in a demo environment.
This guide evaluates the top population health management companies through four criteria that reflect this shift: CMS model readiness, data activation maturity, agentic AI production evidence, and independent analyst recognition.
Best Population Health Management Platforms: A Comparison
Before diving into each vendor, here is how the top population health management companies compare across the criteria that matter most in 2026.
Best Population Health Management Tools: At a Glance
| Vendor | 2026 Analyst Recognition | Unique Capability | Best For |
|---|---|---|---|
| Innovaccer | Black Book #1 AI-Driven Population Health Data Integration, Activation & Analytics (2025 & 2026); Best in KLAS: Data & AI Platform, Payer Analytics, CRM | Direct CMS ACCESS participant (April 13, 2026) with managed program assuming full outcome risk and providing co-management revenue | Enterprise health systems, ACOs, and organizations evaluating ACCESS participation |
| Azara Healthcare | Best in KLAS PHM 4 consecutive years (93.5, 2026) | Largest safety-net PHM platform with 400+ federal/state quality measures optimized for UDS/HEDIS reporting | FQHCs, safety-net providers, community health centers, and clinically integrated networks |
| Epic Healthy Planet | Black Book #1 Core EHR PHM Platform (2025) | Deepest native embedding inside the Epic EHR used by 42% of the acute-care market | Single-EHR Epic health systems |
| Arcadia | Highest KLAS market consideration; 4x Best in KLAS VBC Managed Services | Published dedicated ACCESS readiness framework outlining 5 specific capability requirements | Multi-EHR IDNs and risk-bearing organizations |
| Oracle Health HDI | Large installed base; cloud migration in progress | Enterprise-scale modernization path from the legacy HealthIntent installed base | Existing Oracle Health / Cerner customers |
| Optum | Extensive VBC data assets (100M+ lives) | Vertically integrated modeling and risk adjustment for UHG-affiliated networks | UnitedHealthcare-affiliated networks and large Medicare Advantage plans |
| athenahealth | 5 Best in KLAS awards (2026); strong ambulatory positioning | Network-wide benchmarking and automated outreach embedded directly in athenaOne | Ambulatory-heavy organizations and physician practices |
| Lightbeam | Best in KLAS RPM 2x (93.6, 2025); $5B+ VBC savings | NCQA PHM Prevalidation (Dec 2025) plus deviceless RPM infrastructure | ACOs, MSSP, and Medicare Advantage organizations |
Top Population Health Management Companies and Platforms in 2026
1. Innovaccer
Innovaccer operates the Healthcare Intelligence Platform, organized into four product layers: Gravity (unified data and AI orchestration), Atlas (population health analytics and care management), Story Health by Innovaccer (AI-powered chronic care delivery for heart failure, diabetes, and CKD), and Cured (patient engagement and marketing automation).
The platform manages 80M+ patient records across 130+ organizations, including six of the top 10 U.S. health systems, and powers MEDITECH's Population Insight module for community and regional hospitals running Expanse.
Innovaccer was accepted into the CMS ACCESS model's first cohort as a direct participant on April 13, 2026, one of the few technology companies to hold that distinction. The acceptance is not incidental to the platform's architecture.
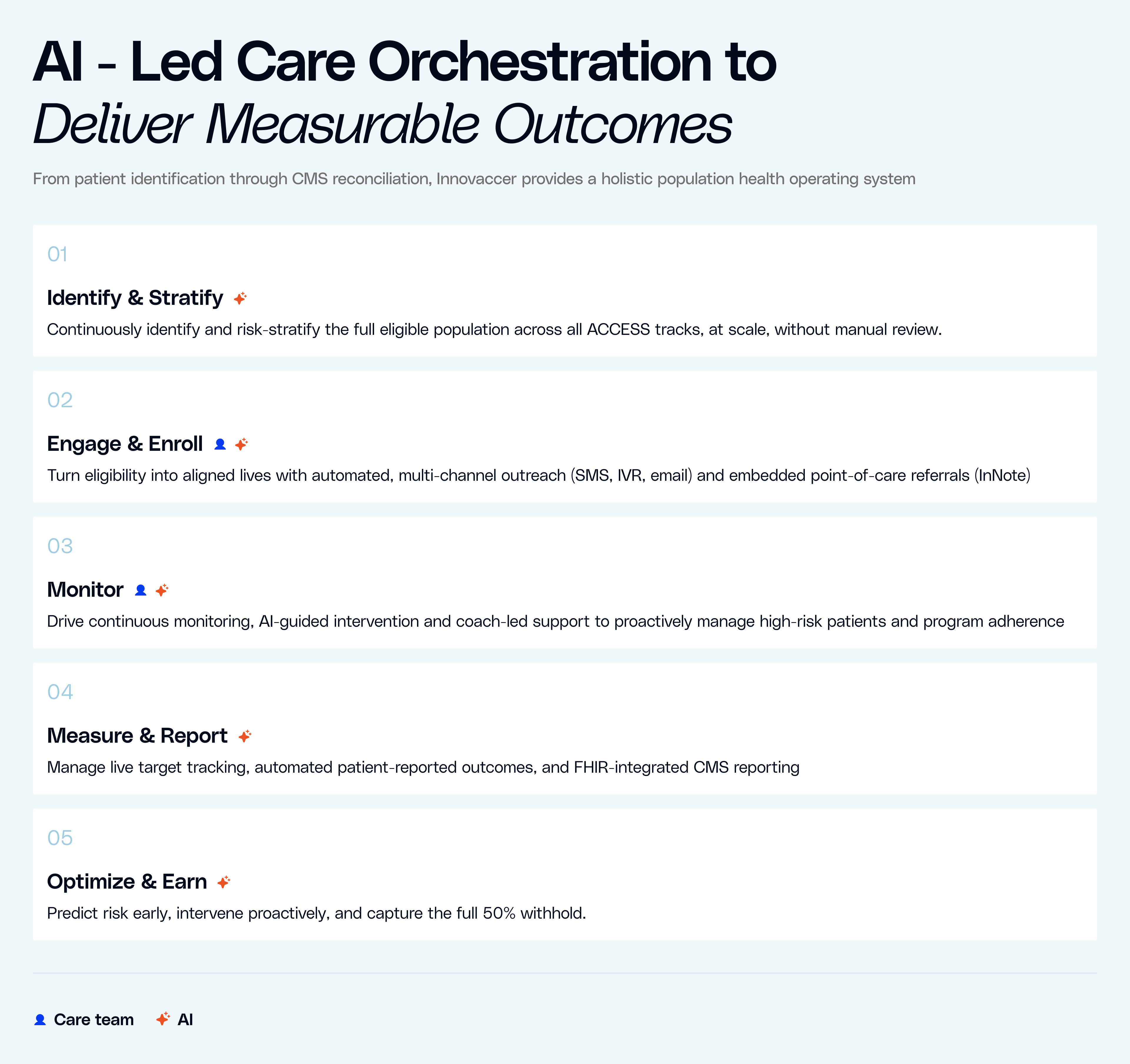
Innovaccer’s chronic care remote delivery maps directly to the ACCESS clinical tracks that represent the model's initial and highest-paying cohorts: early and advanced cardio-kidney-metabolic conditions.
Adaptive Program Intelligence, the care orchestration engine, dynamically scales intervention intensity based on the patient's current condition, moving between AI-only, hybrid, and high-touch human care depending on engagement and clinical signals.
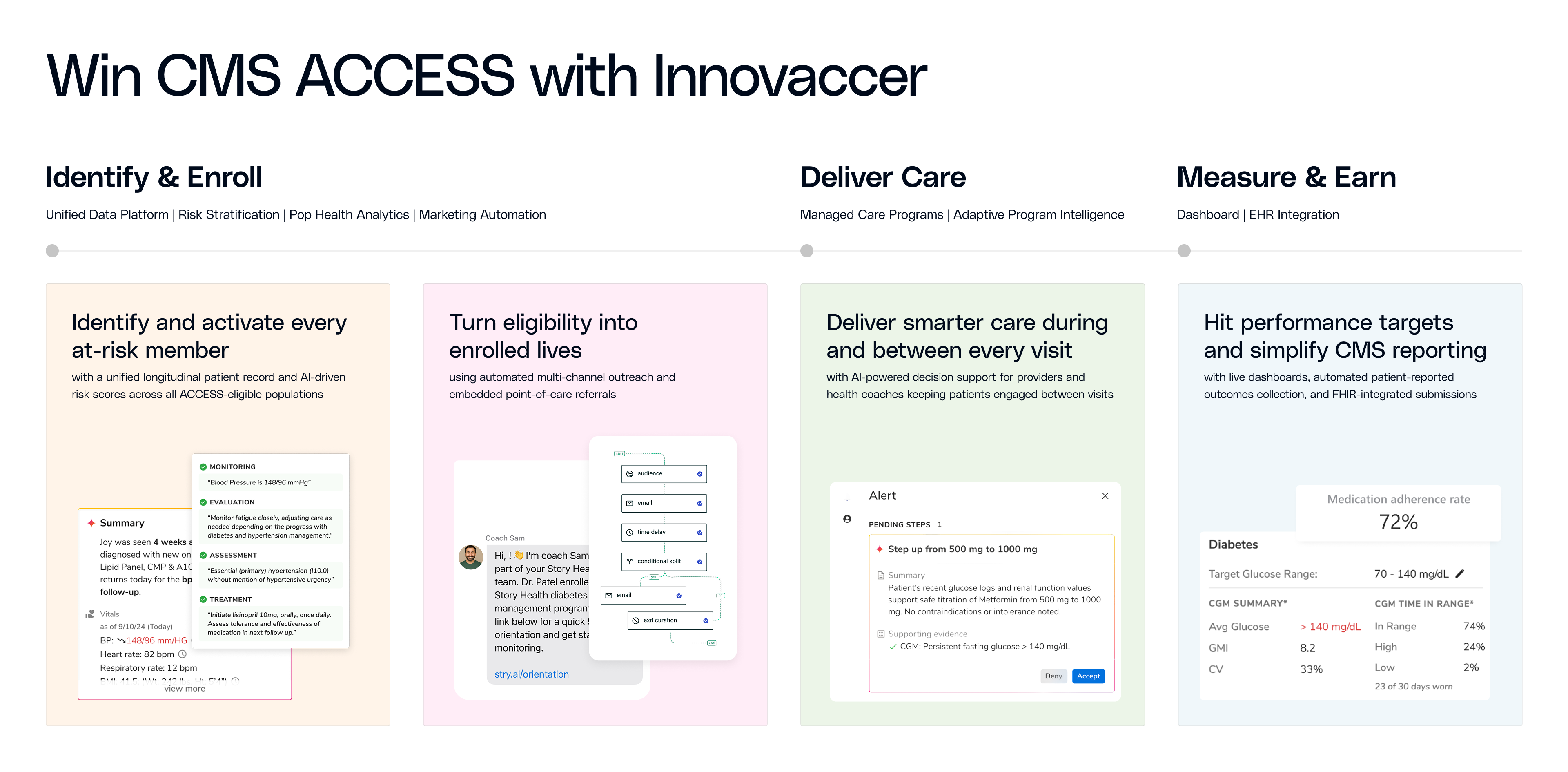
For health systems that want to participate in ACCESS without building RPM, AI engagement, multi-channel outreach, and FHIR CMS API infrastructure from scratch, Innovaccer offers a managed program model where the company enrolls patients, delivers care between visits, and carries the outcome accountability while clinical data flows back to referring providers through Atlas.
Black Book Research ranked Innovaccer #1 in AI-Driven Population Health Data Integration, Activation and Analytics across a 30-vendor field in both 2025 and 2026, evaluated through their 18-KPI framework that specifically measured workflow integration, measure governance, and the ability to convert multi-source data into repeatable operational action.
Innovaccer won 2026 Best in KLAS across three adjacent categories: Data and AI Platform for Providers (93.2), Data Analytics Platform for Payers (90.5), and CRM (90.1, third consecutive year).
The breadth of those wins across provider analytics, payer analytics, and CRM reflects the platform's ability to serve both sides of the value-based care equation within a single architecture, a structural advantage as organizations increasingly manage risk across MSSP, Medicare Advantage, commercial VBC, and now ACCESS and LEAD simultaneously.
The outcomes from Innovaccer's managed care programs reinforce the accreditations: a greater than 60% reduction in hospitalizations and 53% less ED utilization in Intermountain Health's heart failure program, and measurable blood pressure improvements among stage 2 hypertension patients within 90 days across ChristianaCare. The care management copilots have documented 28% reductions in documentation time and 20% improvements in patient engagement in live deployments.
Best for: Enterprise health systems, ACOs, and organizations evaluating ACCESS participation that need a platform spanning data activation, managed care delivery, and outcome accountability.
Explore Innovaccer's Population Health Management Suite |Learn about Innovaccer's CMS ACCESS offering
2. Azara Healthcare
Azara Healthcare is the reigning Best in KLAS for Population Health Management, winning the award four consecutive years (2023 through 2026) with a score of 93.5 in 2026. In February 2025, Azara merged with i2i Population Health under Insight Partners' backing, creating the largest PHM platform serving safety-net providers. The combined entity now covers 25M+ Americans across 1,000+ community health centers, FQHCs, and clinically integrated networks in 43+ states.
Azara's depth in the safety-net segment is unmatched. The platform supports 400+ quality measures across federal and state programs, with particular strength in UDS reporting, HEDIS, and value-based care quality improvement for resource-constrained organizations. The company also launched Smart Summary AI in early 2026, designed to streamline workflows by surfacing critical patient insights for care teams operating with limited staff.
Its consecutive KLAS wins reflect exceptional user satisfaction within that segment, backed by a product built for the specific workflow, regulatory, and resource constraints these organizations face.
Best for: FQHCs, tribal health centers, critical access hospitals, and clinically integrated networks serving underserved communities.
3. Epic Healthy Planet
Epic's Healthy Planet module is the default population health management layer for organizations running Epic's EHR, which holds approximately 42% of the acute-care market. Risk stratification, chronic disease registries, care gap alerts, and quality measure tracking surface directly within the Epic chart, inside the same interface providers use for documentation and ordering. The Cosmos research network adds de-identified data from 250M+ patients for benchmarking and AI-driven research.
The advantage is workflow proximity: providers interact with population health data without leaving their clinical environment, which reduces friction and increases adoption. Epic's PHM capabilities are deeply embedded in the EHR, and the platform's contract performance and quality tracking tools align with value-based care reporting needs.
The consideration for buyers is ecosystem scope. Healthy Planet is not sold as a standalone product and is purpose-built for Epic environments. Organizations running multiple EHRs across their network, or those with significant non-Epic ambulatory footprints, may find that a vendor-agnostic platform provides stronger cross-system data aggregation. For single-EHR Epic shops pursuing value-based care, the native workflow advantage remains substantial.
Best for: Health systems fully committed to the Epic EHR ecosystem seeking deeply embedded population health workflows.
4. Arcadia
Arcadia is a vendor-agnostic analytics and population health platform that consistently ranks among the most frequently considered PHM solutions in KLAS purchase-decision data. The company serves approximately 200 provider, payer, and government customers, including large IDNs and state Medicaid programs. Its 2024 acquisition of CareJourney added AI-powered benchmarking across 300M+ beneficiaries, and in July 2025, Nordic Capital acquired a majority stake, signaling significant growth investment.
Arcadia's cloud-native lakehouse architecture ingests clinical, claims, SDoH, pharmacy, and ADT data from 40+ EHR vendors, providing the multi-source data foundation that ACCESS and LEAD reporting demand.
Arcadia has won four consecutive Best in KLAS awards for Value-Based Care Managed Services and was identified alongside Innovaccer and Epic as a leading PHM vendor in KLAS's population health vendor overview. The company's market consideration rate leads the category, reflecting strong brand awareness and active buyer interest among enterprise-scale organizations. Its KLAS PHM satisfaction scores have room to grow relative to the segment average, a gap worth monitoring as the Nordic Capital investment accelerates product development.
Best for: Multi-EHR enterprises, large IDNs, and risk-bearing organizations that need a vendor-agnostic data platform spanning both payer and provider analytics.
5. Oracle Health Data Intelligence (Formerly Cerner HealtheIntent)
Oracle completed its $28.3B acquisition of Cerner in June 2022, and the HealtheIntent platform now operates as Oracle Health Data Intelligence (HDI) within Oracle's cloud infrastructure. The transition involves migrating the platform to Oracle Cloud Infrastructure while integrating a next-generation clinical AI Agent and voice navigation capabilities launched in August 2025.
Oracle Health HDI retains a significant installed base. Hundreds of health systems built their population health infrastructure on HealtheIntent, and Oracle's enterprise technology ecosystem, including database, cloud, and AI capabilities, positions HDI for modernization at a scale that few pure-play PHM vendors can match. The platform continues to deliver data aggregation, longitudinal record management, and population analytics.
The cloud migration is an active transition, and buyer sentiment reflects that reality. Organizations already invested in the Oracle Health ecosystem have reason to stay engaged as the platform modernizes; the underlying data assets and integration footprint represent years of investment. Organizations evaluating new PHM platforms should weigh the modernization trajectory alongside current implementation timelines and satisfaction signals from recent KLAS data.
Best for: Existing Oracle Health (Cerner) customers evaluating the platform's cloud migration trajectory and AI modernization roadmap.
6. Optum Population Health
Optum occupies a unique position in the population health management landscape. As a subsidiary of UnitedHealth Group, Optum operates at a scale that no other vendor on this list can match: over 100M lives under management, access to one of the largest claims and clinical datasets in U.S. healthcare, and a vertically integrated model that spans care delivery, pharmacy benefits, financial services, and technology.
Optum's population health capabilities are embedded across its technology and services divisions. The company offers analytics, care management tools, risk stratification, and financial modeling capabilities, supported by 1,600+ AI models deployed across the Optum ecosystem. For organizations affiliated with UnitedHealthcare or participating in Optum-managed VBC arrangements, the data connectivity and scale advantages are significant.
The distinction for buyers is that Optum's PHM capabilities function primarily within its own ecosystem rather than as a standalone software product sold to external customers in the way most vendors on this list operate. Organizations outside the UHG network should evaluate whether Optum's tools are accessible and interoperable within their specific care delivery and payer relationships.
Best for: UnitedHealthcare-affiliated networks, large Medicare Advantage organizations, and health systems operating within Optum-managed value-based care arrangements.
7. athenahealth
athenahealth embeds population health management capabilities within its athenaOne platform, serving 140,000+ ambulatory providers. Owned by Bain Capital and Hellman & Friedman, the company earned five Best in KLAS awards for 2026, reinforcing its dominance in the ambulatory market.
athenaOne's network connectivity processes data across its entire customer base to surface benchmarks and best practices, providing ambulatory organizations with population-level insights that would otherwise require enterprise-scale infrastructure. The platform's PHM tools include risk stratification, care gap identification, automated patient outreach, and quality measure tracking. A forthcoming Population Intelligence add-on is expected to bring more robust analytics for organizations managing risk for large populations, including identification of patients with rising risk levels.
athenahealth is best suited for ambulatory-heavy organizations and physician groups that want population health management embedded within their existing EHR and practice management workflows. The platform's strength is seamless integration across clinical, financial, and operational data within the ambulatory setting.
Best for: Ambulatory-heavy organizations and physician practices seeking PHM within an integrated EHR and practice management platform.
8. Lightbeam Health Solutions
Lightbeam is the leading PHM platform purpose-built for ACOs and MSSP participants. Its clients have generated $5B+ in total value-based care savings, with Lightbeam-supported ACOs in Performance Year 2023 earning an average of 17% more than non-Lightbeam ACOs. The company won Best in KLAS for Remote Patient Monitoring two consecutive years (2024 and 2025, scoring 93.6) and was named 2025 Microsoft Healthcare and Life Sciences Partner of the Year.
Lightbeam's RPM model uses a deviceless approach built on text messages and phone calls across 30+ condition-specific programs, lowering enrollment barriers for vulnerable populations who may not have reliable access to connected devices or broadband. This is a critical consideration as ACCESS expands chronic care management to Medicare beneficiaries across all demographics.
Best for: ACOs (MSSP and LEAD-bound), Medicare Advantage organizations, and MSOs that need proven savings track records and deviceless RPM at scale.
How to Evaluate Population Health Vendors Against CMS ACCESS and LEAD
If your organization is evaluating ACCESS participation or preparing for the LEAD transition, your PHM platform is not an abstract technology decision. It is the infrastructure that determines whether you can participate in these models at all.
Five questions will clarify whether your current or prospective platform is ready.
Q1. Has the vendor been accepted as an ACCESS participant or published a readiness framework?
Among the vendors on this list, Innovaccer has been accepted into the ACCESS first cohort (announced April 13, 2026), Arcadia has published a five-capability ACCESS readiness guide, and Lightbeam has achieved NCQA PHM Prevalidation ahead of the LEAD transition. These are verifiable signals of model alignment.
Q2. Does the platform support FHIR-integrated CMS reporting today?
ACCESS requires FHIR-based data submission. Some vendors have this capability in production; others have it on a roadmap. The distinction matters because the first ACCESS cohort launches July 2026.
Q3. Can the platform track patient-reported outcomes at scale?
Two of the four ACCESS clinical tracks (musculoskeletal and behavioral health) measure outcomes entirely through PROMs such as PHQ-9 and GAD-7. Automated collection and submission infrastructure is a requirement, not a feature.
Q4. Does the vendor offer a managed program option that absorbs outcome risk?
ACCESS's 50% withhold structure creates significant downside exposure. Some population health management companies offer end-to-end managed programs where the vendor assumes clinical delivery and outcome accountability while the health system retains FFS billing and earns co-management revenue. Others offer only a platform license where the health system owns program operations and outcome risk. The risk allocation model should factor into your financial analysis alongside platform capabilities.
Q5. Is the platform built for a 10-year horizon?
LEAD's defining feature is no benchmark rebasing over a full decade. Your population health management technology needs to sustain and improve performance over that entire period. Evaluate vendors on their investment trajectory, platform stability, and ability to adapt to policy changes that will inevitably occur across a 10-year model.
Partner with an Accepted CMS ACCESS Participant
Innovaccer is one of the few technology companies accepted into the CMS ACCESS model's first cohort. For health systems participating in ACCESS, that means a path to participation without building the infrastructure from scratch and without carrying the outcome risk.
Your organization keeps its FFS billing, its patient relationships, and earns co-management revenue while Innovaccer delivers the care between visits and reports to CMS.
If ACCESS is on your strategic roadmap for 2026 or 2027, a conversation about how the model maps to your patient population and revenue opportunity is the logical next step. Book a demo.