.png)
Every health system executive managing a chronic care population faces the same constraint: proven care programs that work for hundreds of patients but cannot scale to thousands without proportional headcount.
AI has been positioned as the answer. But the version of AI most care platforms deliver solves the wrong half of the problem.
The State of Clinical AI 2026 from the Stanford-Harvard ARISE network points to a clearer division of labor: AI shows the strongest real-world performance in prediction, monitoring, and workflow tasks at scale, while performance falls in complex, uncertain clinical decision-making.
Monitoring thousands of patients for early pattern shifts is a scale problem. Deciding whether to titrate a heart failure patient’s GDMT based on those signals is a judgment problem. That decision should stay with the treating clinician.
Clinicians reject AI that obscures reasoning and interrupts clinical judgment. The reasons are: poor confidence calibration, limited transparency, and misalignment with how clinical decisions get made. That does not remove AI from care delivery. It defines where AI should contribute and where clinicians must stay in control.
In most care models, that distinction has been strategically interesting but financially avoidable. Under ACCESS, it becomes operationally and economically decisive.
ACCESS Turns the Misalignment Into a Financial Liability
ACCESS encourages organizations to manage qualifying conditions over 12-month periods, ties full payment to track-specific outcome targets, and withholds half of the annual payment for reconciliation after the care period. At ACCESS payment levels, the margin to deliver the same human intensity to every patient does not exist.
Technology can improve monitoring, documentation, and visibility. But if every patient still moves through the same workflow at the same human intensity, the economics break anyway.
Your health coach still spends too much time reviewing stable vitals, confirming adherence, and documenting routine check-ins for patients who are doing fine. Most of that does not require clinical judgment, but it does consume your most limited resource: care team attention.
While your coach is buried in routine reviews, the patient whose glucose has been climbing for three weeks is the one who needs timely clinical intervention. Under ACCESS, delayed intervention is what turns directly into missed outcomes and lost payment.
Solving this requires more than better monitoring or smarter alerts. You need a care model that treats intervention intensity as a variable and adjusts it in real time.
Every patient in your chronic care population needs attention. What varies is the intensity, determined by the critical gaps in each patient's health at any given moment. The question every ACCESS strategy must answer is which patients need your team's direct clinical judgment right now, and which are effectively managed through continuous monitoring until the next clinical gap emerges.
Adaptive Program Intelligence Operationalizes the Difference
Innovaccer’s Adaptive Program Intelligence is built for exactly this gap. It continuously evaluates each patient, adjusts intervention intensity in real time, and routes scale work to the system while routing judgment work to your care team.
For the patients who are stable and engaged, AI-led monitoring handles RPM vitals, adherence signals, and personalized nudges, keeping their health on track by continuously tracking blood pressure, glucose, weight, and medication patterns without pulling your care team into reviews that don't require clinical judgment.
When early risk signals appear, disengagement, biometric drift, missed refills, a health coach steps in to address behavioral, adherence, and social barriers to care. The system continues monitoring, documentation, and scheduling while surfacing a structured alert with context, trend data, and recommended next steps in a unified view.
For the highest-acuity patients, the model escalates to timely clinical intervention: medication titration, care plan changes, and provider coordination. Your clinician receives a structured view of the full picture: recent trajectory, current medications, relevant labs, and guideline-based next steps. They review, apply judgment, and approve. Once the decision is made, the loop closes automatically. The patient receives clear guidance, the care manager reinforces the plan, and the system resumes background monitoring.
.png)
Patients move between these bands dynamically based on real-time signals, with no fixed tiers or rigid assignments. When a patient develops a new condition, Adaptive Program Intelligence layers the new protocol into the existing program instead of forcing a new enrollment, a new care team, and a fragmented experience.
One patient, one continuous relationship, one unified clinical view.
Story Health has already shown that this model can deliver measurable results at scale, including 65% fewer hospitalizations in Intermountain Health heart failure program. But outcomes only tell half the story. The other half is what happens to the patient relationship when care extends beyond your four walls.
Protect Your Patient Relationship
Scaling chronic care under ACCESS means your organization cannot deliver continuous, adaptive management across the full eligible population alone. The model the previous sections describe: AI-led monitoring for stable patients, coach-led engagement for rising risk, clinician-led intervention at inflection points, requires operational capacity most health systems would need 18 to 24 months to build internally.
An ACCESS partner becomes a structural necessity. The question that follows is whether that partnership preserves your providers' clinical authority and visibility or gradually displaces it.
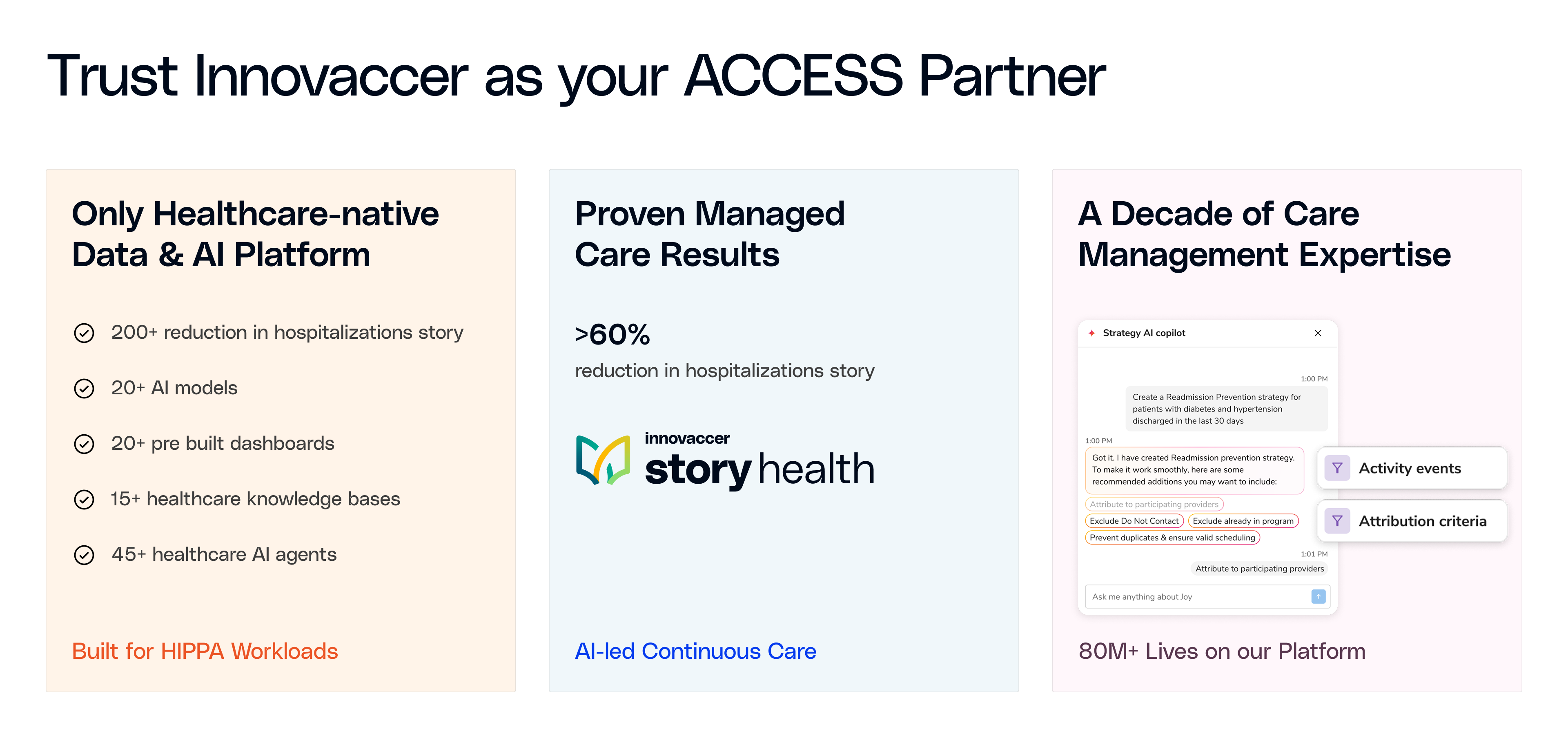
When Innovaccer is your ACCESS partner, your organization does not carry the infrastructure burden, the staffing requirement, or the outcome risk. Innovaccer holds the Part B enrollment, manages clinical delivery through Story Health, and absorbs the full performance risk on Outcome-Aligned Payments.
Your providers continue furnishing services under standard Medicare rules, and referring clinicians can bill the ACCESS co-management service for documented review and care-coordination actions.
Real-time updates on medications, labs, milestones, and care decisions flow back through bidirectional communication and HIE-connected workflows, so your clinical team retains full context throughout the care period.
The partnership adds capacity without displacing authority. Innovaccer operates the ACCESS model. Your organization keeps the patient, the clinical relationship, and the revenue that comes with both.
Smarter Care Wins Under ACCESS
ACCESS rewards care delivery that treat intensity as a variable, allocate AI automation where vigilance matters, reserve clinicians for decisions that require judgment, and keep providers connected to every decision made about their patients.
The organizations that succeed will not be the ones that add more programs or more headcount. They will be the ones that recognize every patient needs continuous attention, but the intensity of that attention must shift in real time based on where the clinical gaps are. ACCESS was built to measure exactly that.
Want to see how you can adopt ACCESS-ready care delivery into your practice? Book a demo